
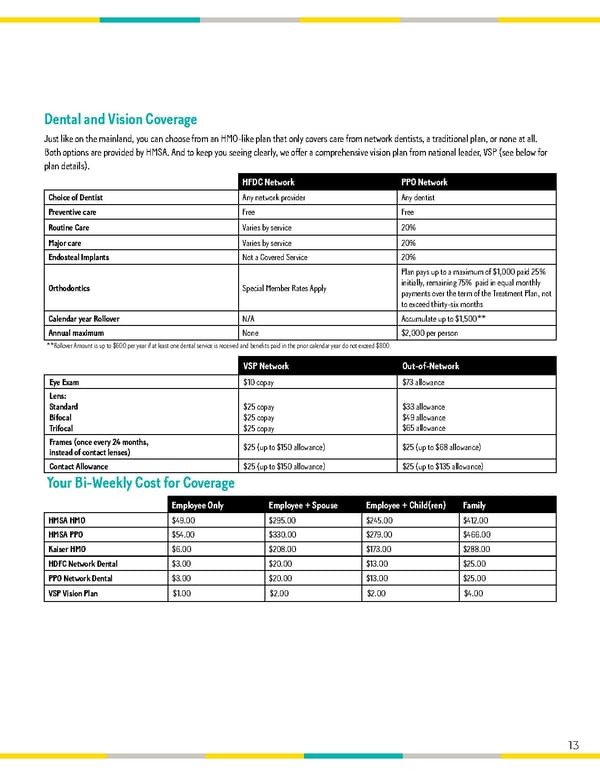
Dental and Vision Coverage Just like on the mainland, you can choose from an HMO-like plan that only covers care from network dentists, a traditional plan, or none at all. Both options are provided by HMSA. And to keep you seeing clearly, we offer a comprehensive vision plan from national leader, VSP (see below for plan details). HFDC Network PPO Network Choice of Dentist Any network provider Any dentist Preventive care Free Free Routine Care Varies by service 20% Major care Varies by service 20% Endosteal Implants Not a Covered Service 20% Plan pays up to a maximum of $1,000 paid 25% Orthodontics Special Member Rates Apply initially, remaining 75% paid in equal monthly payments over the term of the Treatment Plan, not to exceed thirty-six months Calendar year Rollover N/A Accumulate up to $1,500** Annual maximum None $2,000 per person **Rollover Amount is up to $600 per year if at least one dental service is received and benefits paid in the prior calendar year do not exceed $800. VSP Network Out-of-Network Eye Exam $10 copay $73 allowance Lens: Standard $25 copay $33 allowance Bifocal $25 copay $49 allowance Trifocal $25 copay $65 allowance Frames (once every 24 months, $25 (up to $150 allowance) $25 (up to $68 allowance) instead of contact lenses) Contact Allowance $25 (up to $150 allowance) $25 (up to $135 allowance) Your Bi-Weekly Cost for Coverage Employee Only Employee + Spouse Employee + Child(ren) Family HMSA HMO $49.00 $295.00 $245.00 $412.00 HMSA PPO $54.00 $330.00 $279.00 $466.00 Kaiser HMO $6.00 $208.00 $173.00 $288.00 HDFC Network Dental $3.00 $20.00 $13.00 $25.00 PPO Network Dental $3.00 $20.00 $13.00 $25.00 VSP Vision Plan $1.00 $2.00 $2.00 $4.00 13
 California Pizza Kitchen Flipbook Page 12 Page 14
California Pizza Kitchen Flipbook Page 12 Page 14